
Sudden Cardiac Arrest in relation to Ibogaine
Ventricular Tachycardia (VT) and Ventricular Fibrillation(VF)
In Koenig and Hilber study of ibogaine deaths 50% had Ventricular Tachycardia and 17% had Ventricular Fibrillation
With ibogaine there is a risk of a lethal cardiac arrhythmia like “Ventricular-Tachycardia” or “Ventricular-Fibrillation”
These can lead onto a cardiac attack
They can be caused by many things (see below) but of particular interest in relation to ibogaine are; pre-existing heart disease, electrolyte abnormalities such as low potassium, certain medicines, and certain genetic diseases that affect the heart’s ion channels or electrical conduction.
This is because ibogaine causes (hERG) potassium channel inhibition and is known to prolong the QT interval.
Overdose of ibogaine, prolonged QT or electrolyte imbalances can put the patient at risk of VT and VF which can lead to cardiac arrest.
For this reason it is very important to monitor patients QT and QTc interval and get a full 12 Lead ECG EKG and blood panel showing electrolytes prior to admission.
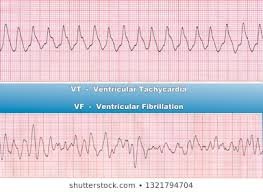
ECG of Ventricular Tachycardia and Ventricular Fibrillation
Ventricular tachycardia (VT)
Ventricular tachycardia (VT) is a fast, abnormal heart rate. Starting in the heart’s lower chambers, called the ventricles. VT is defined as 3 or more ventricular contractions in a row at a rate of more than 100 beats a minute. If VT lasts for more than a few seconds at a time, it can become life-threatening. Sustained VT is when the arrhythmia lasts for more than 30 seconds, otherwise the VT is called non-sustained. The rapid heartbeat doesn’t give your heart enough time to fill with blood before it contracts again. This can affect blood flow to the rest of your body.
What causes VT?
VT is produced in two ways:
- An abnormal heart circuit within the ventricular muscle that is set in motion or triggered (called reentry)
- Abnormal ventricular muscle that becomes self activated (automatically)
VT can occur in an otherwise healthy, or structurally normal heart. It can also occur as a result of damage or scar in the heart from prior heart disease.
VT that occurs in the setting of structural heart disease is more concerning and often can be life threatening. VT that occurs in a structurally normal heart can be benign if it stops on its own.
Any heart condition that results in damage and scar to ventricular muscle can produce VT. It also be caused by an inherited arrhythmia such as long QT syndrome or Brugada syndrome.
VT is often linked to other heart problems that can damage or change normal heart muscle function. Damaged heart muscles can create abnormal electrical circuits that result in VT. You may be more at risk for VT if you have:
- Abnormal heart valves
- Cardiomyopathy
- Heart failure
- Coronary artery disease
- Heart attack
Some types of genetic diseases can also lead to VT. These include:
- Conditions that cause abnormal heart muscle, such as hypertrophic cardiomyopathy
- Diseases that can get inside the heart muscle, such as sarcoidosis
- Diseases that alter properties within the heart rhythm itself such as long QT syndrome or brugada syndrome
In some cases, VT occurs when there are no other heart problems.
Symptoms of VT
Fast beating heart that may only last for a few seconds. Longer episodes may be dangerous. The heart beats so fast that it struggles to get enough blood to the rest of your body.
Symptoms of VT include:
- Fast heartbeat or a fluttering feeling in the chest (palpitations)
- Dizziness
- Lightheadedness
- Chest pain
- Neck tightness
- Shortness of breath
- Fainting
- Cardiac arrest
In some cases, there are no symptoms at all
Treatment for sustained ventricular tachycardia
- Sustained ventricular tachycardia often requires urgent medical treatment, as may to lead to sudden cardiac death.
- Treatment involves restoring a normal heart using a defibrillator or with a treatment called cardioversion.
- Defibrillation can be done using an automated external defibrillator (AED).
- Cardioversion is done in a hospital setting using a machine that monitors your heart rhythm before and after shocks are delivered. In this procedure, medical professionals shock your heart using paddles, an automated external defibrillator (AED) or patches on your chest.
- There are also medications that can be used like Lidocaine (avoid amiodarone as it is QT prolonging). Be careful though as Lidocaine can kill someone in torsades.
Ventricular Fibrillation
Ventricular fibrillation (V-fib) is a dangerous type of arrhythmia, or irregular heartbeat. It affects the heart’s ventricles. In a healthy heart, your blood pumps evenly in and out of these chambers. This keeps blood flowing throughout your body.
Ventricular fibrillation is an arrhythmia that starts in your ventricle. This occurs when the electrical signals that tell your heart muscle to pump cause your ventricles to quiver (fibrillate) instead. The quivering means that your blood is not pumping blood out to the rest of your body. In some people, V-fib may happen several times a day. This is called an “electrical storm.”
Sustained V-fib can lead to sudden cardiac arrest (SCA) and/or sudden cardiac death (SCD). It needs immediate medical attention.
Causes of ventricular fibrillation
The cause of ventricular fibrillation is not always known but it can occur with certain medical conditions. V-fib most commonly occurs during an acute heart attack or just after. When heart muscle does not get enough blood flow, it can become electrically unstable and cause dangerous heart rhythms. A heart that has been damaged by a heart attack or other heart muscle damage is vulnerable to V-fib.
Other causes include heart failure, heart valve disease, electrolyte abnormalities such as low potassium, certain medicines, and certain genetic diseases that affect the heart’s ion channels or electrical conduction.
The most common risk factors include:
- A weakened heart muscle (cardiomyopathy)
- An acute or prior heart attack
- Genetic diseases such as long or short QT syndrome, Brugada disease, or cardiomyopathy
- Certain medicines that affect heart function
- Electrolyte abnormalities
Symptoms of ventricular fibrillation
Symptoms of V-fib include:
- Near fainting or transient dizziness
- Fainting
- Acute shortness of breath
- Cardiac arrest
How is ventricular fibrillation treated?
There are 2 stages of treatment for V-fib. The first tries to stops your V-fib immediately to restore a blood pressure and pulse. The second stage focuses on reducing your chances of developing V-fib in the future. Treatment includes:
- CPR. The first response to V-fib may be cardiopulmonary resuscitation (CPR). This will keep your blood moving to important organs.
- Defibrillation. This is an electrical shock that is delivered to the chest wall to restore normal rhythm. It is often critical to perform immediately once V-fib is diagnosed.
- Medicines Sometimes medicines are given immediately after V-fib to help control and prevent another episode.
- Implantable cardioverter defibrillator (ICD). This is a device that is implanted within the body to monitor for V-fib. If detected, it can automatically deliver an energy shock to restore normal heart rhythm.
Torsades de Pointes – Most common rhythm
In the Koenig and Hilber study, out of 19 ibogaine deaths 33% had Torsades de Pointes
- Problems that occur with the heart’s rhythm are known as arrhythmias.
- When the heart beats faster than usual, as in a case of torsades de pointes, it is called tachycardia.
- Torsades de pointes is French for “twisting of points” and refers to when the heart’s two lower chambers (ventricles), beat faster than the upper chambers, which are known as the atria.
- Most cases of torsades de pointes resolve on their own without treatment. However, it can develop into ventricular fibrillation, which can lead to cardiac arrest and may even be fatal.
- Torsade de pointes is a distinctive form of polymorphic ventricular tachycardia (VT) characterized by a gradual change in the amplitude and twisting of the QRS complexes around the isoelectric line (see the image below).
- Torsade de pointes, is associated with a prolonged QT interval, which may be congenital or acquired.
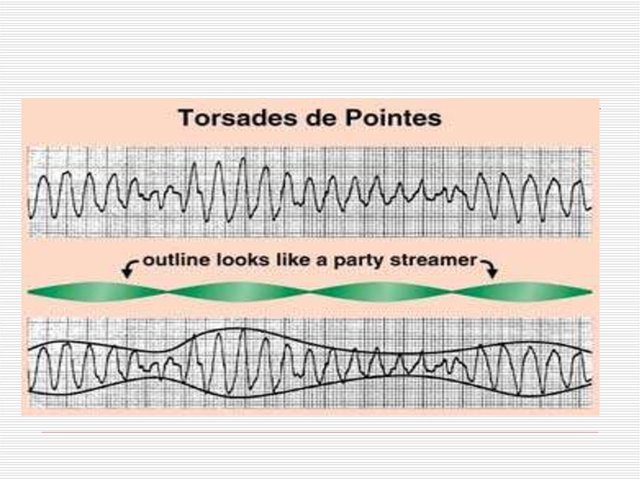
ECG of Torsades de Pointes
Common causes for torsades de pointes include drug-induced QT prolongation and less often diarrhea, low serum magnesium, and low serum potassium or congenital long QT syndrome. It can be seen in malnourished individuals and chronic alcoholics, due to a deficiency in potassium and/or magnesium.
-
Torsades de pointes — ‘twisting of the points.’ In this arrhythmia, your heart’s two lower chambers (ventricles) beat fast and chaotically, making the waves on an ECG monitor look twisted. Less blood is pumped out from your heart, so less blood reaches your brain, causing you to faint suddenly and, often, without any warning.
If a torsades de pointes episode is short — lasting less than one minute — your heart can correct itself and you regain consciousness on your own. However, if a torsades de pointes episode lasts longer, it can result in a sudden fainting spell followed by a full-body seizure. If the dangerous rhythm does not correct itself, then a life-threatening arrhythmia called ventricular fibrillation follows.
-
Ventricular fibrillation. This condition causes the ventricles to beat so fast that your heart quivers and ceases pumping blood. Unless your heart is shocked back into a normal rhythm by a defibrillator, ventricular fibrillation can lead to brain damage and sudden death.
It’s now known that long QT syndrome might explain some cases of sudden death
• TdP always requires ICU care.
• TdP is treated with IV Magnesium



QT Prolongation and Ibogaine
The QT interval is a measurement made on an electrocardiogram used to assess some of the electrical properties of the heart. It is calculated as the time from the start of the Q wave to the end of the T wave, and approximates to the time taken from when the cardiac ventricles start to contract to when they finish relaxing. In short its a way to monitor your hearts activity and health.
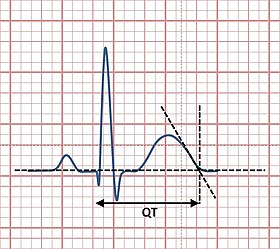
The picture above shows a normal QT, a prolonged QT would look as if it was “stretched out” when this happens there is a risk that the various parts of the heart may not fire in the right order, which can cause BIG PROBLEMS. See below:
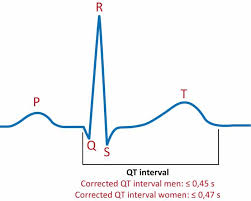
Need to correct the QT interval
The QT interval shortens at faster heart rates, and lengthens at slower heart rates. Since the QT interval is influenced by the heart rate, it needs to be corrected. A correction formula is required to come up with a corrected QT or QTc which estimates the QT interval at a heart rate of 60 beats per minute (bpm). This allows comparison of QT values over time at different heart rates.
What is the importance of the QTc?
The QTc, when prolonged means that the heart muscle takes longer than normal to recharge between beats. To have a prolonged QTc means one is at increased risk of arrhythmias, which when severe, can lead to syncope, cardiac arrest or sudden death. Prolonged QTc can be due to congenital defects, electrolyte imbalance, or medications
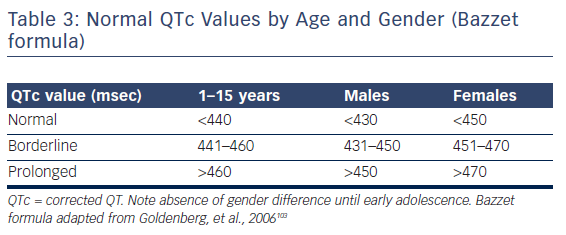
A QTc of >470 and >450 ms was associated with an increased risk of sudden death, for women and men, respectively, and a QT or QTc interval exceeding 500 ms can be regarded a significant risk for torsade de point. At least eight of such cases have been described in relation to ibogaine since 2008.
- QTc values ranged from minor prolongation of only 480 ms to a dramatic one with more than 700 ms in duration.
- Except for one case the prolongation of the QT interval subsequently evolved into ventricular tachycardia (VT) and/or ventricular fibrillation (VF). In many cases this developed into torsade de point (TdP) arrhythmias was observed.
- Only in one case the lack of arrhythmia occurrence was reported. However, in this case the QT interval was only minimally prolonged (480 ms).
In Koenig and Hilber study of ibogaine deaths 75% had a QTc above 593 and 25% QTc between 480-498
In all instances proper medical interventions could’ve saved the lives of these people.
Methods to correct the QT interval
There are four formulae to correct the QT interval, namely Bazett, Fredericia, Framingham and Hodges, of which Fredericia is the one we will use in the example below and is referred to as the QTcF or QTcFrid.
The QTcF may be arrived at manually or generated automatically by the ECG machine.
Below we will outline how you work out a QTcF manually.
Which ECG machine?
Some 12 lead ECG machines have an automatic QTc reporting feature and are preferred. But the QTc can still be worked out on a 3 lead ECG.33% Torsades de Pointes















Talk to us!
Our knowledgeable volunteers will share their personal experience of ibogaine with you and advise you on how to find a good clinic.
+34 643280060
For a free call back:
Text, Whatsapp, Telegram app or email us!
brain@ibogainehotline.co
Or by clicking the blue speech bubble to the right of the screen to chat to us right now!
Join our facebook group and get first hand advice from people who have already made their journies with ibogaine www.facebook.com/groups/1521724148001426/
Like our Facebook page www.facebook.com/ibogainehotline


The Anti-Addiction Drug Ibogaine and the Heart: A Delicate Relation
Read More

Entheo-Science – Jeff Kamlet: Ibogaine Safety
Read More

Detoxing from Methadone with Ibogaine – Clare Wilkins Psychedelic Science Conference 2017
Read More

Dr Fred’s Ibogaine Safety Presentation at the European Ibogaine Forum
Read More

Ibogaine Adverse Reactions & Safety – Jamie Mac – Ibogaine / Cardiac Nurse – Notes from the European Ibogaine Forum
Read More

Welcome to Ibogaine Hotline
Read More

Dutch study on the longterm benefits of ibogaine treatment for drug addiction
Read More